

Artificial Disk Replacement in the Lumbar Spine
In artificial disk replacement, worn or damaged disk material between the small bones in the spine (vertebrae) is removed and replaced with a synthetic or "artificial" disk. The goal of the procedure is to relieve back pain while maintaining more normal motion than is allowed with some other procedures, such as spinal fusion.

Total artificial disk replacements are mechanical devices that simulate spinal function.
CHARITÉ artificial disk. Reproduced with permission from DePuy Spine, Inc. © 2007 DePuy Spine, Inc. All rights reserved.
Lumbar Fusion and Artificial Disk Replacement
Although it is estimated that 70% to 80% of people will experience low back pain at some point in their lives, most will not need surgery to improve their pain. Surgery is considered when low back pain does not improve with conservative treatment.
For patients who have exhausted nonsurgical options and are still in pain, lumbar fusion surgery remains the most common option for treating low back pain. Fusion is essentially a "welding" process. The basic idea is to fuse together the painful vertebrae so that they heal into a single, solid bone.
While many patients are helped by lumbar fusion, the results of the surgery can vary. In addition, some patients whose fusion surgeries heal perfectly still end up with no improvement of their back pain.
Some doctors believe that the failure to improve after fusion surgery is because fusion prevents normal motion in the spine. For this reason, artificial disk replacement—which aims to preserve normal motion—has emerged as an alternative treatment option for low back pain.
Artificial disk replacement initially gained FDA approval for use in the U.S. in 2004. Over the past several years, numerous disk replacement designs have been developed and are currently being tested.

These x-rays, taken from the side, show patients treated with (left) lumbar spinal fusion, and (right) artificial disk replacement.
(Right) Reproduced from Mathur S, Jenis LG, An HS: Surgical Management of Chronic Low Back Pain: Arthrodesis, in Jenis LG, ed: Low Back Pain: Monograph Series.(Left) Reproduced from Jenis LG: Surgical Management of Chronic Low Back Pain: Alternatives to Arthrodesis, in Jenis LG, ed: Low Back Pain: Monograph Series. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005.
Who Is a Candidate for Disk Replacement?
To determine if you are a good candidate for disk replacement, your surgeon may require a few tests, including:
- Magnetic resonance imaging (MRI) scans
- Discography
- Computed tomography (CT) scans
- X-rays
Information from these tests will also help your surgeon determine the source of your back pain.
Artificial disk replacement is not appropriate for all patients with low back pain. In general, good candidates for disk replacement have the following characteristics:
- Back pain caused by one or two problematic intervertebral disks in the lumbar spine
- No significant facet joint disease or bony compression on spinal nerves
- Body size that is not excessively overweight
- No prior major surgery on the lumbar spine
- No deformity of the spine (scoliosis)
Surgical Procedure
Most artificial disk replacement surgeries take from 2 to 3 hours.
Your surgeon will approach your lower back from the front through an incision in your abdomen. With this approach, the organs and blood vessels must be moved to the side. This allows your surgeon to access your spine without moving the nerves. Usually, a vascular surgeon assists the orthopaedic surgeon with opening and exposing the disk space.
During the procedure, your surgeon will remove your problematic disk and then insert an artificial disk implant into the disk space.
Disk Design
Some disk replacement devices comprise the nucleus (centre) of the intervertebral disk while leaving the annulus (outer ring) in place, although this technology is still in an investigative stage.
In most cases, total artificial disk replacements substitute both the annulus and nucleus with a mechanical device that will simulate spinal function.
There are several different disk designs. Each is unique, but all maintain a similar goal: to reproduce the size and function of a normal intervertebral disk.
Some disks are made of metal, while others are a combination of metal and plastic, like joint replacements in the knee and hip. Materials used include medical grade plastic (polyethylene) and medical grade cobalt chromium or titanium alloy.
Your surgeon will talk with you about which disk design is best for you.
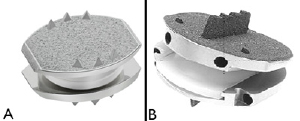
Examples of total artificial disk replacements.
A. CHARITÉ artificial disk. Reproduced with permission from DePuy Spine, Inc. © 2007 DePuy Spine, Inc. All rights reserved. B. ProDisc-L prostheses. Reproduced with permission from Synthes, West Chester, PA.
Recovery
In most cases, you will stay in the hospital for 1 to 3 days following artificial disk replacement. The length of your stay will depend upon how well-controlled your pain is and your return to function.
In most cases, patients are encouraged to stand and walk by the first day after surgery. Because bone healing is not required following artificial disk replacement, the typical patient is encouraged to move through the midsection. Early motion in the trunk area may lead to quicker rehabilitation and recovery.
You will perform basic exercises, including routine walking and stretching, during the first several weeks after surgery. During this time, it is important to avoid any activities that cause you to hyperextend your back.
Outcomes
Most patients can expect improvement of lower back pain and disability in weeks to months following surgery. Studies show that disk replacement improves, but does not eliminate pain. Before your surgery, it is important to talk with your surgeon about realistic expectations for pain relief.
Research on the Horizon
The future of artificial disk replacement technology will likely include advancements in the design of implants and tools for diagnosing the source of pain, as well as the development of ways to return the disk to normal function without the insertion of any biomechanical device.
Although no longer considered a new technology, the development of artificial disk replacement is more recent than that of lumbar fusion. Follow-up studies to 10 years have shown satisfactory outcomes in a carefully chosen patient population. Despite the theoretical advantages of preserving motion, some studies have not shown a clear advantage of artificial disk replacement over lumbar fusion. Research continues on the outcomes of the procedure.










